Abstract #010: The Clinical Cell-Cycle Risk Score is Associated with Metastasis After Radiation Therapy and May Identify Men with Prostate Cancer Who Can Forgo Combined Androgen Deprivation Therapy
Jonathan Tward, MD, PhD,1 Lauren Lenz, MS,2 Darl D. Flake II, PhD,2 Saradha Rajamani, PhD,2 Carl Olsson, MD,3 Deepak A. Kapoor, MD,3 Constantine Mantz, MD,4 Stanley L. Liauw, MD,5 Tatjana Antic, MD,5 Neal Shore, MD,6 Dan Albertson, MD,7 Jonathan Henderson, MD,8 Steve P. Lee, MD,9 Hiram A. Gay, MD,10 Jeff Michalski, MD,10 Arthur Hung, MD,11 David Raben, MD,12 Isla Garraway, MD, PhD,13 Michael S. Lewis, MD,13 Paul L. Nguyen, MD,14 David T. Marshall, MD, MS,15 Steven Stone, PhD,2 Todd Cohen, MD,2
1Huntsman Cancer Institute, University of Utah, Salt Lake City, UT; 2Myriad Genetics, Inc., Salt Lake City, UT; 3Advanced Radiation Center of New York, New Hyde Park, NY, and Integrated Medical Professionals, North Hills, NY; 421st Century Oncology, Fort Meyers, FL; 5University of Chicago Medical Center, Chicago, IL; 6Carolina Urologic Research Center, Myrtle Beach, SC; 7University of Utah Department of Anatomic Pathology and Molecular Oncol- ogy, Salt Lake City UT; 8Regional Urology, LLC, Shreve- port, LA; 9Long Beach VA Medical Center, Long Beach, CA; 10Department of Radiation Oncology, Washington University, St. Louis, MO; 11Oregon Health & Science Uni- versity, Portland, OR; 12University of Colorado, Aurora, CO; 13Greater Los Angeles-VA Medical Center, Los Angeles, CA; 14Dana-Farber Cancer Institute, Boston, MA; 15Medical University of South Carolina, Charleston, SC
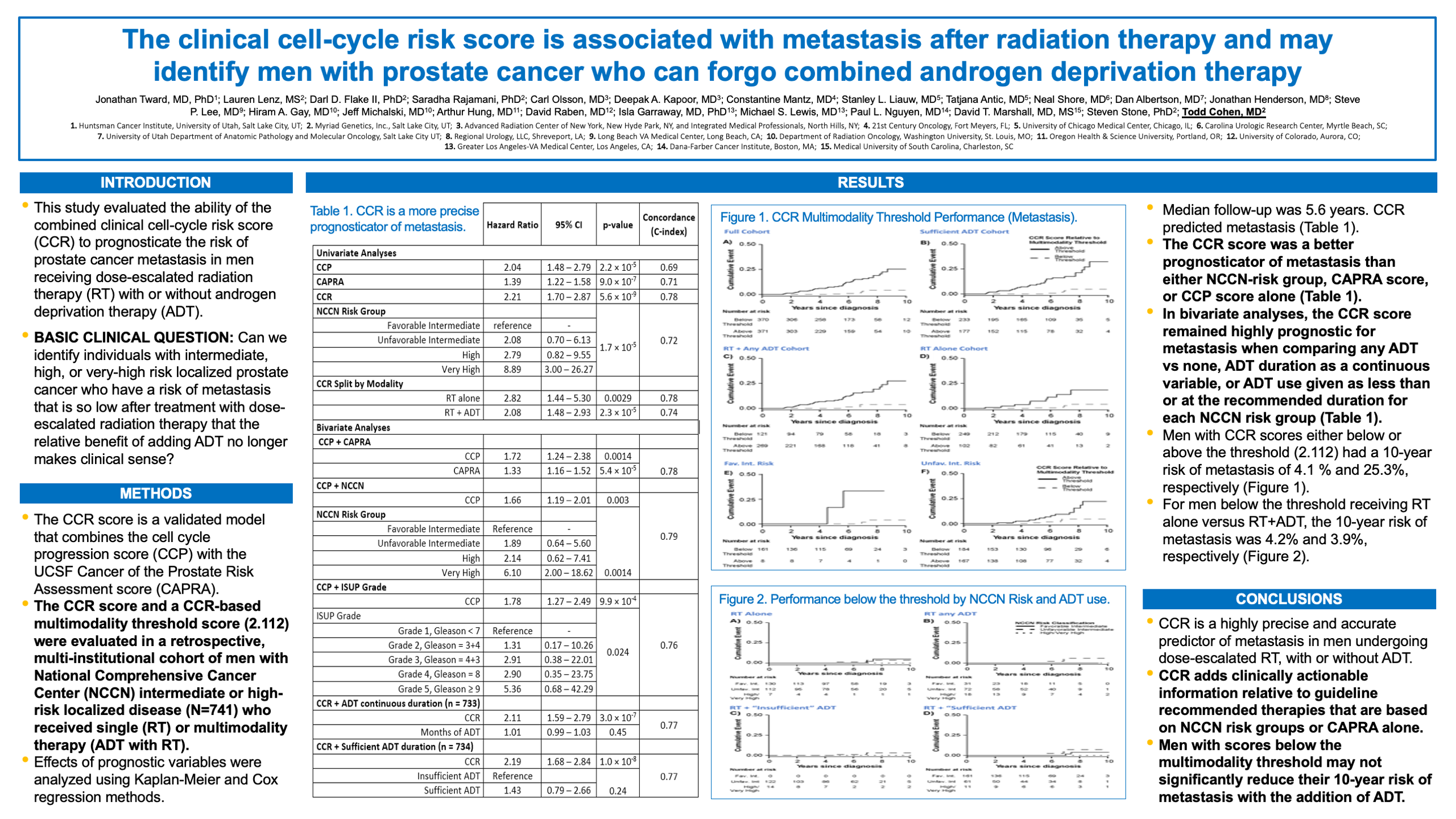
Introduction: This study evaluated the ability of the com- bined clinical cell-cycle risk score (CCR) to prognosticate the risk of prostate cancer metastasis in men receiving dose- escalated radiation therapy (RT) with or without androgen deprivation therapy (ADT).
Methods: The CCR score is a validated model that com- bines the cell cycle progression score (CCP) with the UCSF Cancer of the Prostate Risk Assessment score (CAPRA). The CCR score and a CCR-based multimodal- ity threshold score (2.112) were evaluated in a retro- spective, Multi-Institutional cohort of men with National Comprehensive Cancer Center (NCCN) intermediate- or high-risk localized disease (N=741) who received single (RT)- or multimodality therapy (ADT with RT). Effects of prognostic variables were analyzed using Kaplan-Meier and Cox regression methods.
Results: Median follow-up was 5.6 years. CCR predicted metastasis [hazard ratio (HR) 2.21, 95% Confidence Interval (CI) 1.70-2.87, p<0.001]. The CCR score was a better prognosticator of metastasis (C-index 0.78) than either NCCN-risk group (C-index 0.72), CAPRA score (C-index 0.71), or CCP score (C-index 0.69) alone. In bivariate analyses, the CCR score remained highly prog- nostic for metastasis when comparing any ADT vs none (HR 2.19, 95% CI 1.62 to 2.97, p<0.001), ADT duration as a continuous variable (HR 2.11, 95% CI 1.59-2.79, p<0.001), or ADT use given as less than or at the recom- mended duration for each NCCN risk group (HR 2.19, 95% CI 1.68-2.84, p<0.001). Men with CCR scores either below or above the threshold (2.112) had a 10-year risk of metastasis of 4.1 % and 25.3%, respectively. For men below the threshold receiving RT alone versus RT+ADT, the 10-year risk of metastasis was 4.2% and 3.9%, respectively.
Conclusions: CCR is a highly precise and accurate predictor of metastasis in men undergoing dose-escalated RT, with or without ADT. CCR adds clinically actionable information relative to guideline recommended therapies that are based on NCCN risk groups or CAPRA alone. Men with scores below the multimodality threshold may not significantly reduce their 10-year risk of metastasis with the addition of ADT.