Robert G. Uzzo, MD, MBA, FACS, presented “Guidelines Based Management of Localized and Locally Advanced RCC” during the 28th Annual Perspectives in Urology: Point Counterpoint on November 16, 2019 in Scottsdale, Arizona.
How to cite: Uzzo, Robert G. “Guidelines Based Management of Localized and Locally Advanced RCC” November 16, 2019. Accessed Jul 2025. https://grandroundsinurology.com/guidelines-based-management-of-localized-and-locally-advanced-rcc
Guidelines Based Management of Localized and Locally Advanced RCC – Summary:
Robert G. Uzzo, MD, MBA, FACS, discusses the updated American Urological Association (AUA) guidelines on renal cell carcinoma (RCC) and notes the remarkable advances made in the past 20 years. He emphasizes the importance of careful patient selection and the key role of systemic therapy.
Abstract
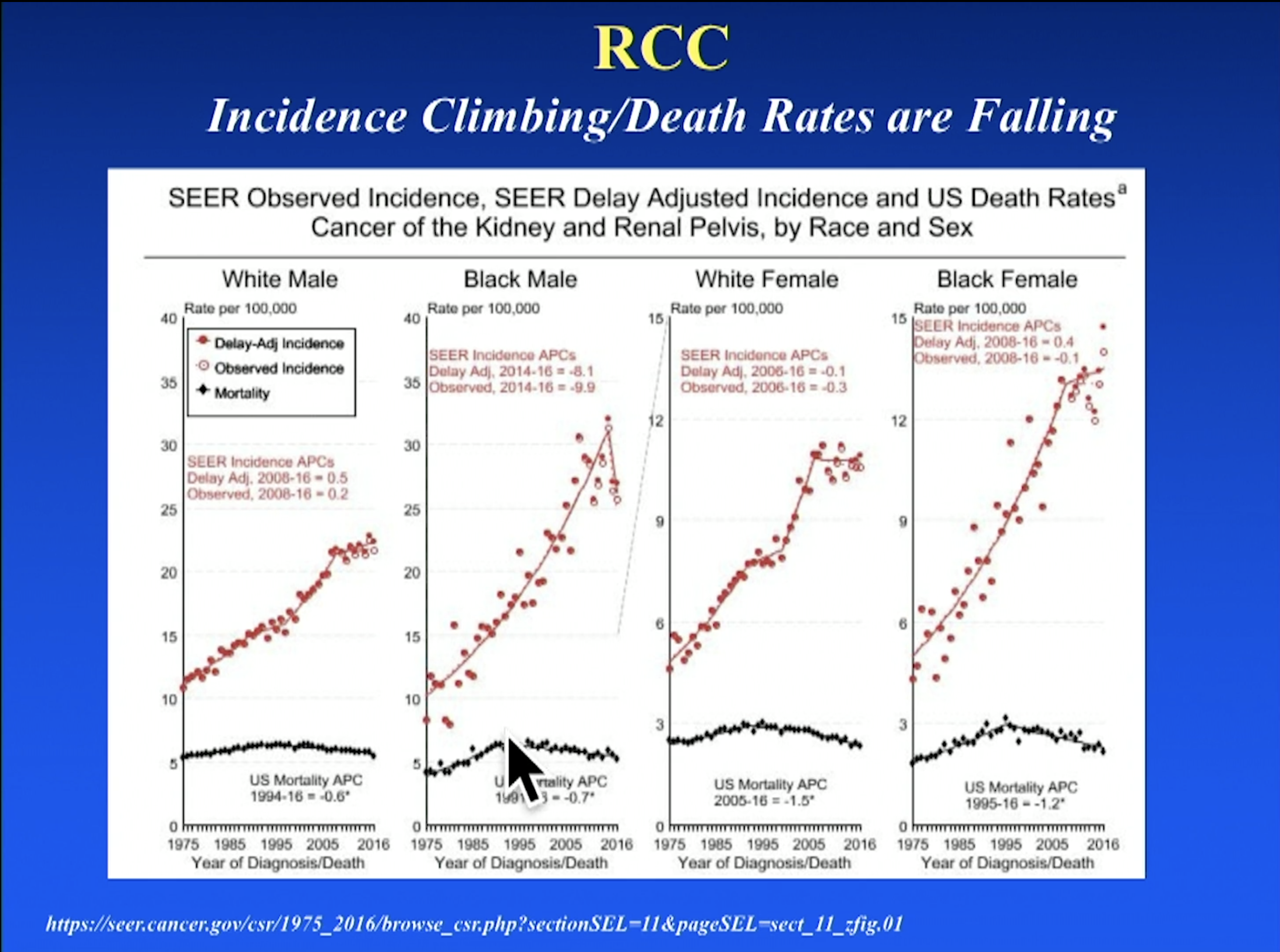
From 1950 until 2000, the average survival and the response rate to therapy in metastatic kidney cancer patients remained static at 10 months and 5%, respectively. Since 2000, these numbers have increased to 50 months and 60%, even as RCC incidence has increased. This does not seem to be due to surgical advancements since there have been few significant surgical trials and urologists are relying on procedures like cytoreductive nephrectomy less and less. Meanwhile, 15 medications have been approved since 2005 in the area of systemic therapy for RCC. The updated AUA guidelines for RCC management reflect the development, or lack thereof, of these two treatment modalities.
The 2017 AUA RCC guidelines emphasize tailoring treatment to individuals. This includes encouraging genetic counseling for younger patients, but is particularly important in the area of risk assessment. Urologists must communicate to their patients the common and serious urologic and non-urologic morbidities of each treatment pathway and highlight the importance of patient age, comorbidities, and life expectancy. Not all patients are good candidates for surgery. Research indicates that partial nephrectomy will more likely lead to complications in patients with more complex tumors, and cytoreductive nephrectomy only works with well-selected patients. Fortunately, advances in systemic therapy mean that there are options for patients who should not get surgery or be put on active surveillance.
Patient response to systemic therapies like axitinib, pembrolizumab, and sunitinib is common, early, and ongoing. The CARMENA trial demonstrated that sunitinib alone was not inferior as a treatment to nephrectomy followed by sunitinib. If a patient would be unable to quickly get on systemic therapy after surgery because of performance or frailty, then they should not get surgery. The AUA still recommends surgery for well-selected patients, but its role is being refined in the era of such effective systemic therapy.
About Perspectives in Urology: Point Counterpoint
Perspectives in Urology: Point Counterpoint (PCP) is an annual, multi-day, CME-accredited conference devoted to discussing and debating the latest topics in men’s health and general urology, as well as management of bladder, renal, and both localized and advanced prostate cancer. More than didactic lectures, the conference’s format includes debates, point-counterpoint discussion panels, and unique case-based presentations. Dr. Uzzo presented this lecture during the 28th PCP in 2019. Please visit this page in order to register for future PCP meetings.
ABOUT THE AUTHOR
Robert G. Uzzo, MD, MBA, FACS, is Chairman of the Department of Surgery at Fox Chase Cancer Center–Temple University Health System, where he is the G. Willing “Wing” Pepper Endowed Professor of Surgery. He also serves as the organization’s Deputy Chief Clinical Officer and President of the Medical Group. Regionally, Dr. Uzzo is the Chair of the Fox Chase/Einstein Urologic Institute of Southeastern Pennsylvania and the Executive Director of the nation’s second-largest urologic quality collaborative (the Pennsylvania Urologic Regional Collaborative, or PURC). Dr. Uzzo’s work focuses on the surgical management of genitourinary malignancies.
Dr. Uzzo graduated summa cum laude and valedictorian from Union College’s accelerated 6-year biomedical program in Schenectady, New York. He attended Cornell University Medical College in New York City, where he was a New York State Finalist for the Rhodes Scholarship Competition. He completed general surgical training followed by urologic surgical training at New York Hospital-Cornell Medical Center and Memorial Sloan-Kettering Cancer Center. He was an American Foundation for Urological Diseases Scholar in Urological Oncology and completed both Oncological and Renal Transplantation Fellowships at the Cleveland Clinic under Dr. Andrew C. Novick.
Dr. Uzzo’s primary research has been in renal cell carcinoma (RCC), with a special focus on clinical decision making, surgical management, and adjuvant therapies. Dr. Uzzo has been involved in multiple national and international trials in kidney cancer. He has authored over 400 peer-reviewed articles and chapters in urologic oncology. He is a Diplomat of the American Board of Urology, a Fellow of the American College of Surgeons, and an elected member of both the prestigious American Association of Genitourinary Surgeons and the Clinical Society of GU Surgeons.