Riccardo Autorino, MD, PhD, FEBU, presented “Robotic Surgical Systems in Urology: What’s in the Pipeline?” at the Jackson Hole Seminars on February 7, 2018 in Jackson Hole, Wyoming.
How to cite: Autorino, Riccardo. “Robotic Surgical Systems in Urology: What’s in the Pipeline?” February 7, 2018. Accessed Mar 2026. https://grandroundsinurology.com/Robotic-Surgical-Systems-in-Urology/
Summary:
Riccardo Autorino, MD, PhD, FEBU, reviews the assets and limitations of the robotic systems currently available for clinical urological applications, especially the da Vinci system. He describes the global scene of emerging systems, such as the REVO-I and the avatera-System, as well as multiple systems under development.
Robotic Surgical Systems in Urology: What’s in the Pipeline? – Transcript
Click on slide to expand
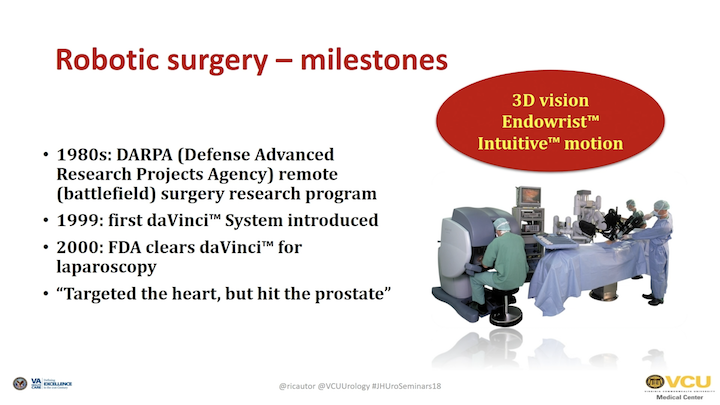
Robotic Surgery – Milestones
As you know, the history with body surgery—I started many years ago.
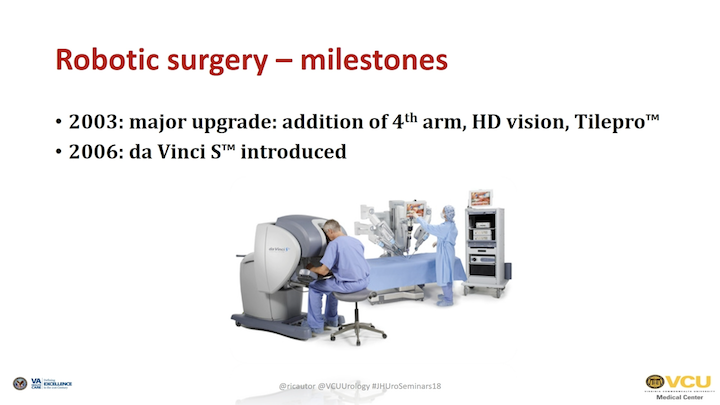
Robotic Surgery – Milestones #2
Over these many years that has been – there have been some major upgrades of the current da Vinci system.
Robotic Surgery – Milestones #3
We pass from different generations of the robot, each one better with some technical enhancement compared to the previous one.
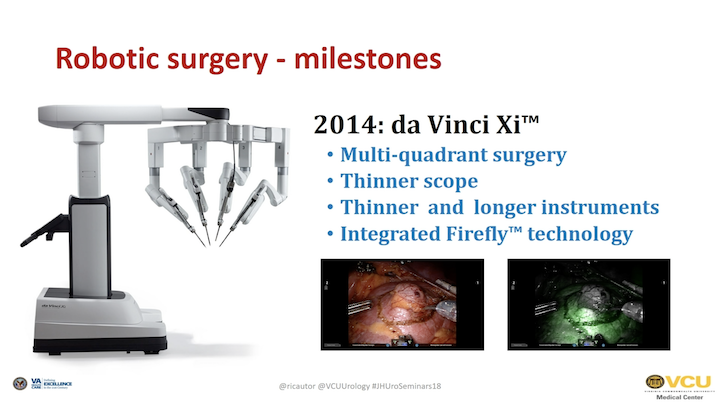
Robotic Surgery – Milestones #4
The last one is the one that came out about three years ago, the Xi, which allows multi-quadrant surgery, thinner instrument—longer instrument—and thinner instrument- and a thinner scope, and it allows, also, to have some integrated Firefly technology.
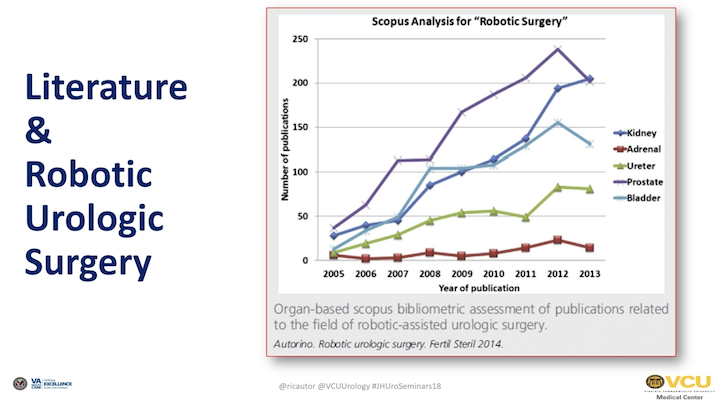
Literature and Robotic Urologic Surgery
As we have been using robotic surgery, also the literature on robotic surgery in urology has certain increased, and certainly, the robot has impacted majorly our field.

Urologic Oncology
If you think about this, prostatectomies were done mostly open when the robot came out. Now, about 80%, or that is one of the estimates, of prostatectomies done in the U.S. are done robotically, as you probably already know.
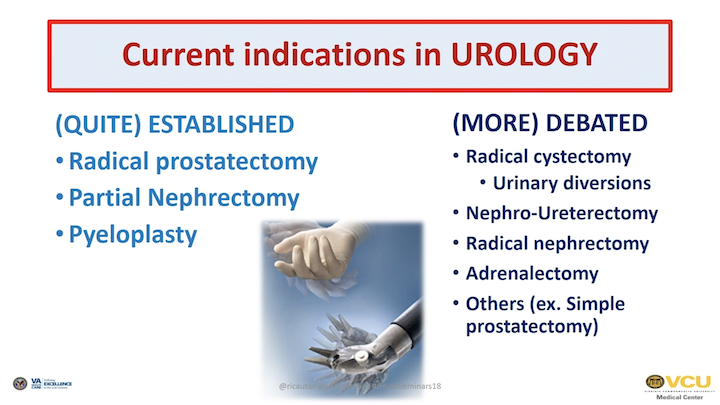
Current Indications in UROLOGY
There are current indications for urologic applications of robotic surgery. Some of them are quite established. Some others are more debatable, or questionable, if you like it.
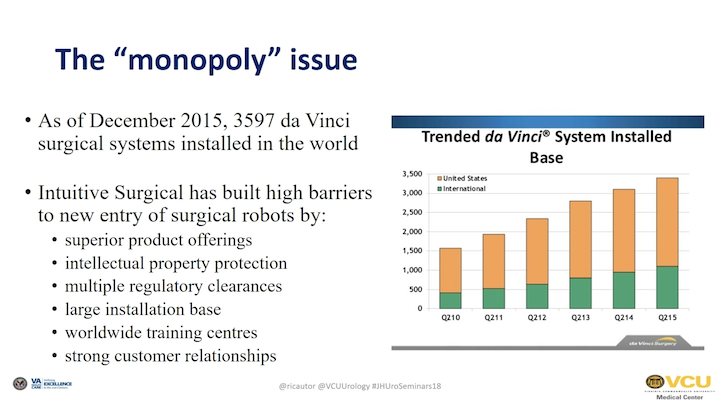
The “Monopoly” Issue
Certainly, one big issue with robotic surgery is that we have only one company. So, it’s a monopoly that is in charge to control the market, and they—the robotic system installed in the world from Intuitive has been exponentially grown over the years. And with time, they also now, you know, they put up high barriers against the entry of other surgical robots, just because they have a very good product. First of all, certainly. And then, there are some patent issues, regulatory clearances, the also worldwide training centers. They are very customer, relationship—very good relationship with customers, very strong presence on the field, and therefore, it’s difficult to compete with such a company.
However…
However, things might change soon, because in a very short time, some of the patents they have—they will expire. And, this can generate intriguing, stimulating research that has been done in different parts of the world. So, things might change, in other words.
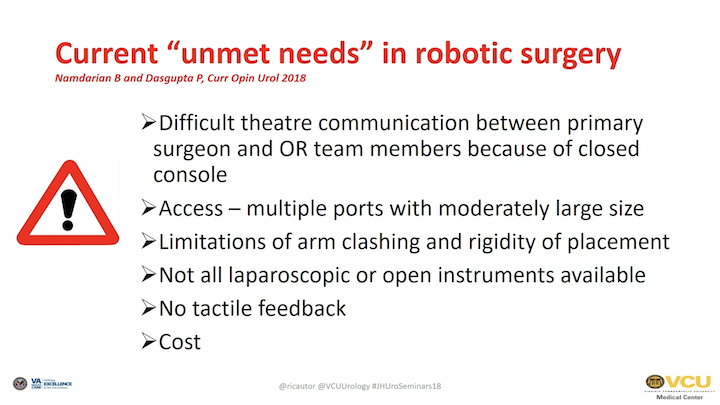
Current “Unmet Needs” in Robotic Surgery
And certainly, if the da Vinci is a very good toy, on the other side, there are some drawbacks, and these are listed here in this paper from Dr. Dasgupta. There is some difficult communication between the consult surgeon and the OR team. You see – – multiple ports. There is also some degree of clashing, and also, you don’t have the wide variety of instruments that you have with open or laparoscopic surgery. Still, there is an issue of not having any tactile feedback. And last but not least, the cost is still very sky high to buy and maintain a robot.
Beyond da Vinci
What are the other options that are basically on the market?
Senhance™ – TransEnterix Inc
One, you might have seen these before, is the Senhance system. This was bought by TransEnterix, which is a North-Carolina-based company. The technology, however, was developed in Italy by—in Northern Italy, and then was bought—the company was bought from this American company. And they are trying, now, to commercialize the product. I’m not aware of many.
Senhance – TransEnterix Inc – video
They probably have sold a handful number of systems because the cost is still high, but the main future of this system, as you can see from this video, is that basically, they have a—the surgeon is seated at a console. First of all, the big difference with da Vinci, each arm is separated by the other, so they are all independent, and there can be an advantage in terms of port placement. In terms of where the—as you can see, however, the instruments they are more similar to laparoscopic instruments and robotic, and the wrist instrument that we use nowadays. The surgeon is sitting here. Also, the handles are more similar to laparoscopy, so they are not ergonomically as comfortable with the da Vinci. And, the surgeon position is certainly comfortable, but the way he moves the image is by using a 3D glasses, and there is a high tracking system. One of the distinctive features of this system is that there is some tactile feedback, so the surgeon can feel when he touches a structure in the belly, and this is probably a major – probably a significant improvement, as is shown here in this video. And again, this is the way it works. The surgeon moves the head and he can zoom on one part of the field.
Senhance – TransEnterix Inc – clinical (non-urology) data
This has been used clinical, not in urology, for OB-GYN cases, and also for colorectal surgery.
Senhance – TransEnterix Inc – clinical (non-urology) data #2
Groups in Italy published on these, and that’s because the company who developed the technology was based in Italy, so they had collaboration with surgeons from that area of the world.
Senhance – TransEnterix Inc – clinical (non-urology) data #3
And in terms of our specialty, just some preclinical study in pigs with partial nephrectomy has been done.

REVO-I
This is also another thing that is not—so that one is on the market in the—already in the U.S. This one is not. It’s going to be on the market soon, probably in Korea this year, price to be determined. I asked Dr. Koon Rha from Yonsei, who is the major—the PI—on the clinical development of this system. It is still a master slave system. You have a very—it looks like the intuitive one, so you have a four-arm robotic patient cart, the tower, and the console. And, the instruments are usable, more usable than the one from the Intuitive.
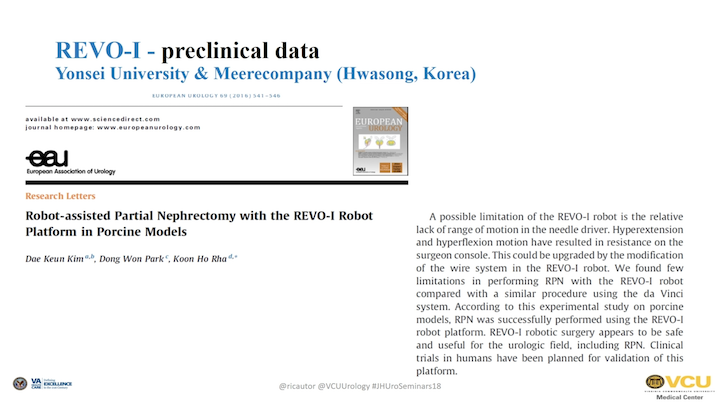
REVO-I – Preclinical Data
They initially published a pre-clinical study in the pig model.

REVO-1 – Retzius-sparing Radical Prostatectomy Video Clip
And they also—they have done also a—again, it might not work, or it might work. But, this was a small video clip showing a Retzius-sparing radical prostatectomy. So, there is some—so, they did a clinical series on this, showing the clinical feasibility and safety of the device. That probably will receive the Korean FDA approval this year, and will be on the market there. When it will be on the market here? That, I’m not sure. As you can see, it’s very, probably, not quite as good as the Intuitive one, but very similar.
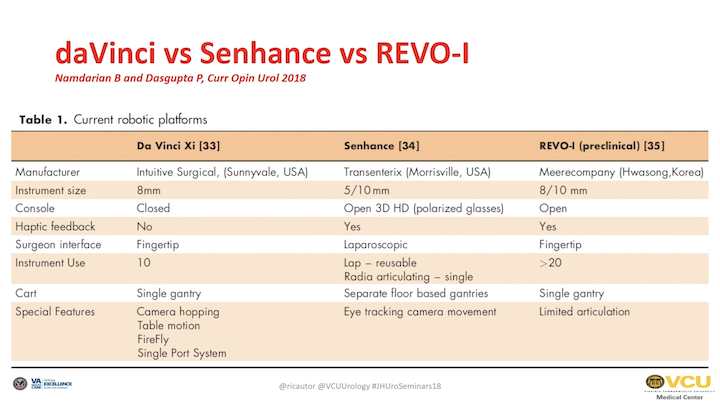
da Vinci vs Senhance vs REVO-I
That is a table summarizing basically, the three systems, again, the three systems that are on the market. As you can see, we talked about—well, I would point out the size of the instruments that are different here. Here, for the fact of having different arms that are separated, and the reusable instruments that are completely reusable on the Senhance, which can be cost-effective in the long-term. And also, for the REVO compared to the da Vinci, you can use the instrument more than 20 times. So also, that is some—there might be some cost saving.
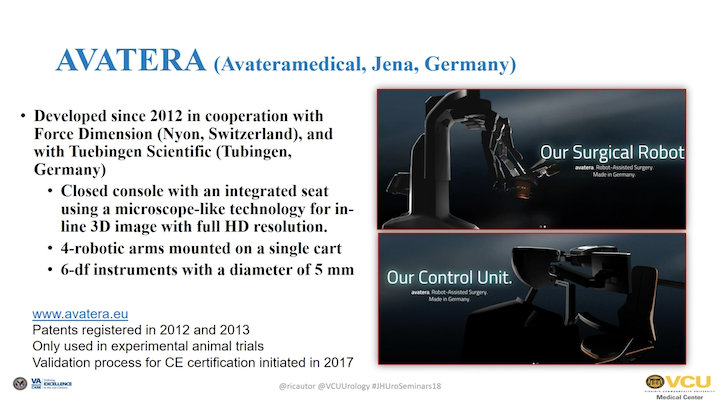
AVATERA
Then, there are some other systems that are still under development.
So, one is the one developed by a company called Avatera in Germany. This has been—they have been working on this for a few years now. These are a couple of pictures, as you see, there a console with an integrated seat. They have a 3D HD image. Now, they have the full robot mounted on a single cart. The instrument—they have six degree of freedom, and they are 5-mm in diameter.
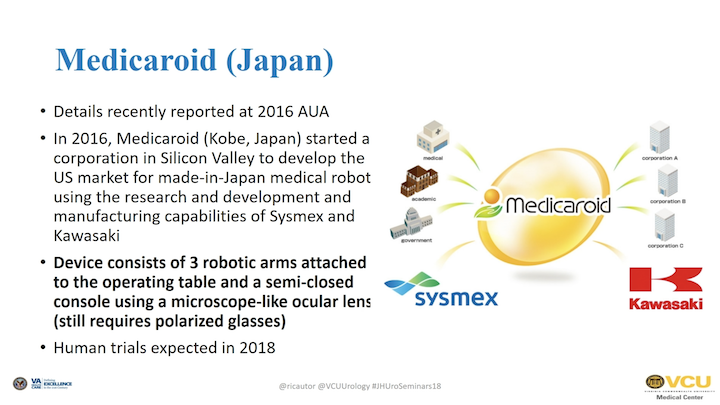
Medicaroid (Japan)
In Japan, there is another company, Medicaroid, that is basically a joint company, but from Kawasaki and Sysmex. They also have a factor in Silicon Valley. They are working on a robot, which seems to be a robot with three robotic arms that are mounted to the operative table, a microscope-like technology, and also, for these human trials are expected for later this year.
Medtronic Robot
Then, the one that is also ongoing, in terms of a work in progress, I would say is the one that is being developed by Medtronic, and this is actually technology that was initially started in Germany.
Medtronic Robot #2
What happened is that Covidien bought the license for commercial use. Then, Medtronic bought Covidien, and basically, they are working now on the tenth prototype. They plan to start clinical trials in India, and eventually, launch the device later this year in the United States. We’ll see.

Verb Surgical
Last, again, this is joint effort by Google and Johnson & Johnson in a company called Verb Surgical. There is no way to find any information on this. This is very top secret, so the only thing that we know that they are working on that. So, I’m not sure what else to tell you about that.
da Vinci Robotic Single Port Surgery: Recent Advances
I will then move on with my presentation by showing you some advances in the field of single port surgery.

EAU
As you know, single site, or single port surgery has been very exciting for many surgeons worldwide a few years ago. And then, the interest for this, this was a study that we did a few years ago. Fernando was also involved, a big effort by all of these centers showing basically the technical feasibility but also the technical challenges of doing these laparoscopically.

VESPA (da Vinci Single-Site)
The robot could be the answer to advance the field, and actually Intuitive initially proposed this system, which is called VESPA, or da Vinci Single-Site. That is the commercial name. Basically, the instruments are curved instruments that go through—that can triangulate through the—by entering the abdomen and allowing to, basically, have a triangulation, because as you know, the main problem with single-site surgery is that instruments are parallel, and that can be challenging. And, we did this animal study when I was on clinic, and showing with testes in the animals, as you can see, a big limitation, again, is the fact that the instruments are basically laparoscopic instruments, not—they don’t have any articulation.

EAU #2
Some centers in Europe have done clinical—this was really commercialized mostly for cholecystectomy for general surgeons. Then some urologists, adopted for pyeloplasty, and they have done some—they have done cases with good outcomes, comparable to standard multi-port surgery. This is a video from Professor Guazzoni from Milan, and for the sake of time probably I can move on, but again you see the same image that you were seeing in the pig model, basically, but this is in a patient. So, in the hands of good surgeons, it can be done with this platform.

da Vinci SYMPTOM System—1st Generation (SP999)
The further advance from the Intuitive has been the so-called da Vinci SP system. We worked on this study. It was a clinical study that we published a few years ago. They had done a nephrectomy and radical prostatectomy cases were done, the cases were done in France actually, was a giant effort by the – – Group and the University of Lille.
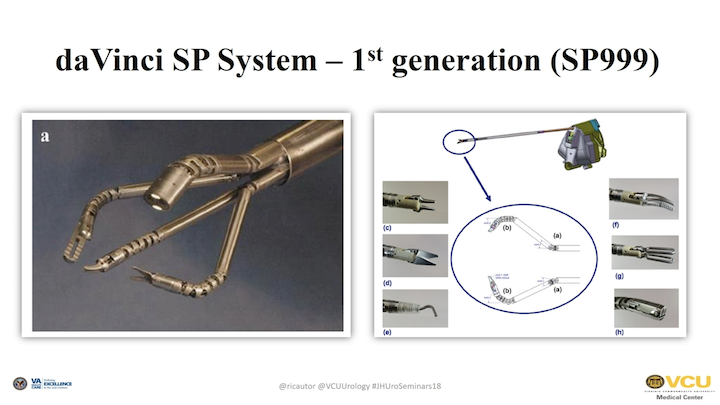
da Vinci SYMPTOM System—1st Generation (SP999) #2
And basically, the idea was to have a single port that you can introduce into the abdomen, and then have a camera and instrument that goes through the port and work. These instruments are different from the ones we use with standard body surgery, because they have an additional site where the instrument can bend, and therefore, you can have triangulation while you are inside. And to allow this, you need the specific patient cart that I will show in a second, a newer version of this.
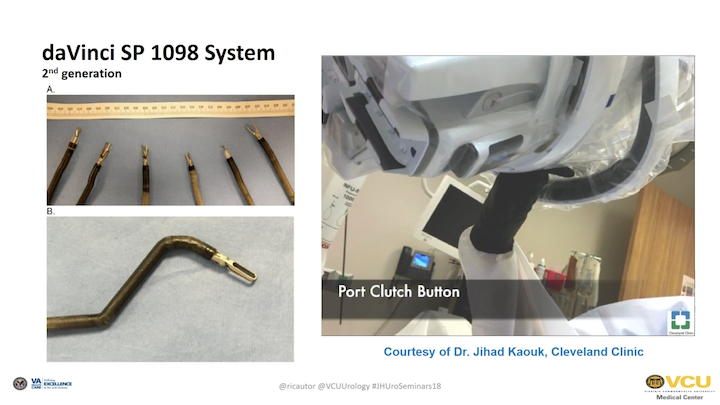
Single Port Surgical System
That is already a second generation, and basically, also they improved the quality of the instruments, and you can see this is a patient cart that is very similar to the current Xi patient cart, and this, however, allows to put all of the instruments as you can see. I think it is worth seeing this video, specifically, because you can basically put all of the instruments through the same cannula that I will show in a second here. And this is – as you can see, it is a single—in this case, it’s a lab working on a cadaver. And basically, you can put the port through the—this is the port, which is about 25mm, and through this port, the port is similar to the trocar that we use for the Xi. It’s different channels, however, that is the difference, and through this you can put the—there is an obturator, so you can put the port through the obturator. And then, you can basically—each of these is the docking site for each of the instruments. So the—it is something still in progress, but it is basically very—almost ready to—the market, and we will see. It was supposed to come out on the market a couple of years ago. It didn’t, so maybe, probably, commercial business for that.
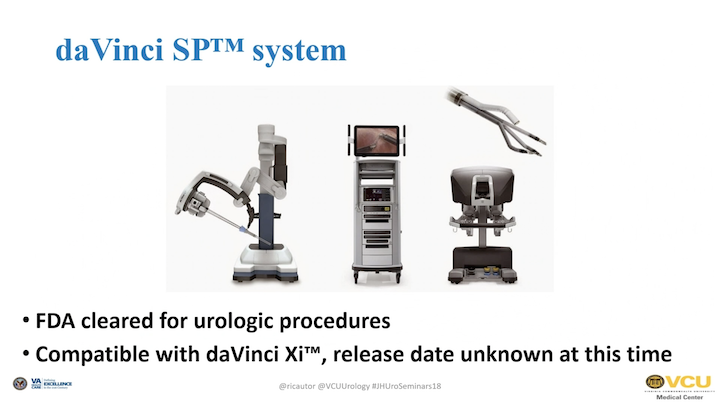
da Vinci SP system
But, as you can see, this is what you would probably see later this year.
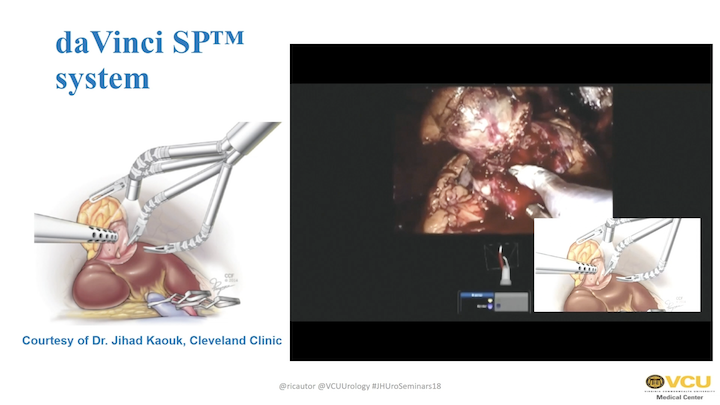
da Vinci SP system #2
And again, this is just a video clip to show how the technology allows you to, basically, perform a surgery with the same, you know, steps of a standard partial nephrectomy. This is a partial nephrectomy case done here. This is the column from the kidney. So, getting access to the kidney, performing the resection of the tumor, performing the – – and all done with the—again, with a single access point. Of course, then the question is, “Do you believe in single access versus multi-port surgery?” That is another question, but technology, basically, is almost ready to. And again, this is not the last prototype, the last generation of this. So, moving on. Again, this is going to be—this is already FDA cleared and is comparable. You need to have an Xi to use this.

Beyond da Vinci SP

SPORT Titan Medical*
Other companies are working on this. The SPORT is a Canadian-based company that has been working on this forever. And was supposed to lead the market, but it never did. The same—similar concept as you see here.

SPORT Titan Medical- video clip
But, this is a small video clip of this. But again, this is more similar to the Senhance, to the one from TransEnterix. So, we did the consult surgeon sits here. He has 3D glasses, and the instruments are more similar to laparoscopic instruments, so probably not a step forward in a good direction.
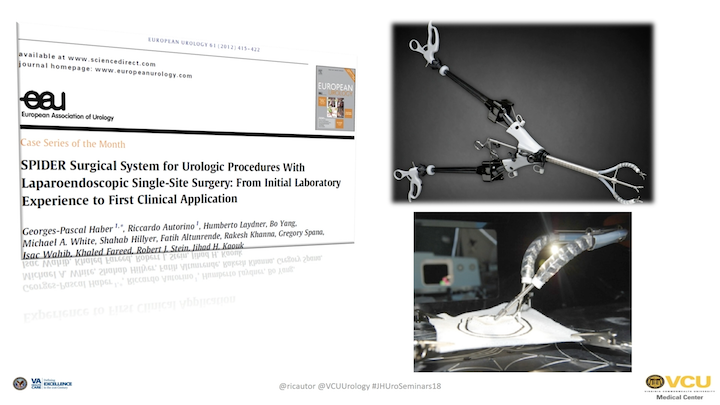
EAU #3
This is something else that we worked a few years ago called SPIDER. Was considered for – – single-site surgery, and now we have an advanced version of it called Surgibot from the same company.
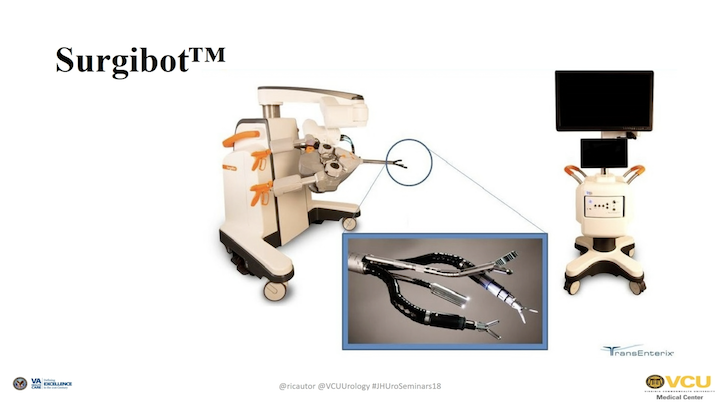
Surgibot
But, still not sure if this is going to be very successful, because it’s still not a perfect system.

Take home – Robotic Surgical Systems in Urology: What’s in the Pipeline?
To give you some take-home messages, I think several robots will probably hit the market in the next 5, 10 years. The da Vinci, the Intuitive, has set very high technical standards, and unfortunately, all these devices will need to compared to what we have now, which is standard. We will see how it goes. And, the implementation of all of these instruments will depend not only by their approval, but also by the clinical applicability, the cost, and ultimately, we will also need to understand if they can translate in better patient outcomes. And, if you want to read more about this there is this review, which was mainly done by Dr. Rassweiler from Germany.
Main Reference
Did a lot of effort, a huge really systematic review including all of the knowledgeable on this—in this field. Thank you again for your attention.
ABOUT THE AUTHOR

Riccardo Autorino, MD, PhD, FEBU, is the Director of Clinical Outcomes Research for the Glickman Urological and Kidney Institute at the Cleveland Clinic in Cleveland, Ohio.His main clinical interest is the minimally-invasive treatment of urologic cancers and benign urologic diseases using robotic-assisted surgery.